Pudendal Nerve Entrapment Reference Center
A Robotic Solution for
A Robotic Solution for
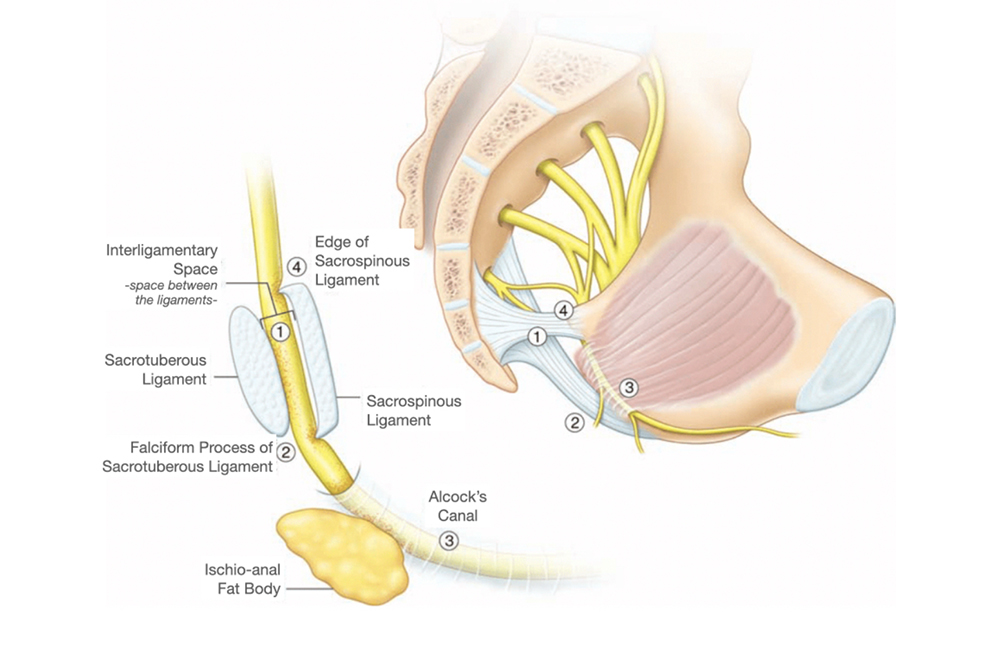
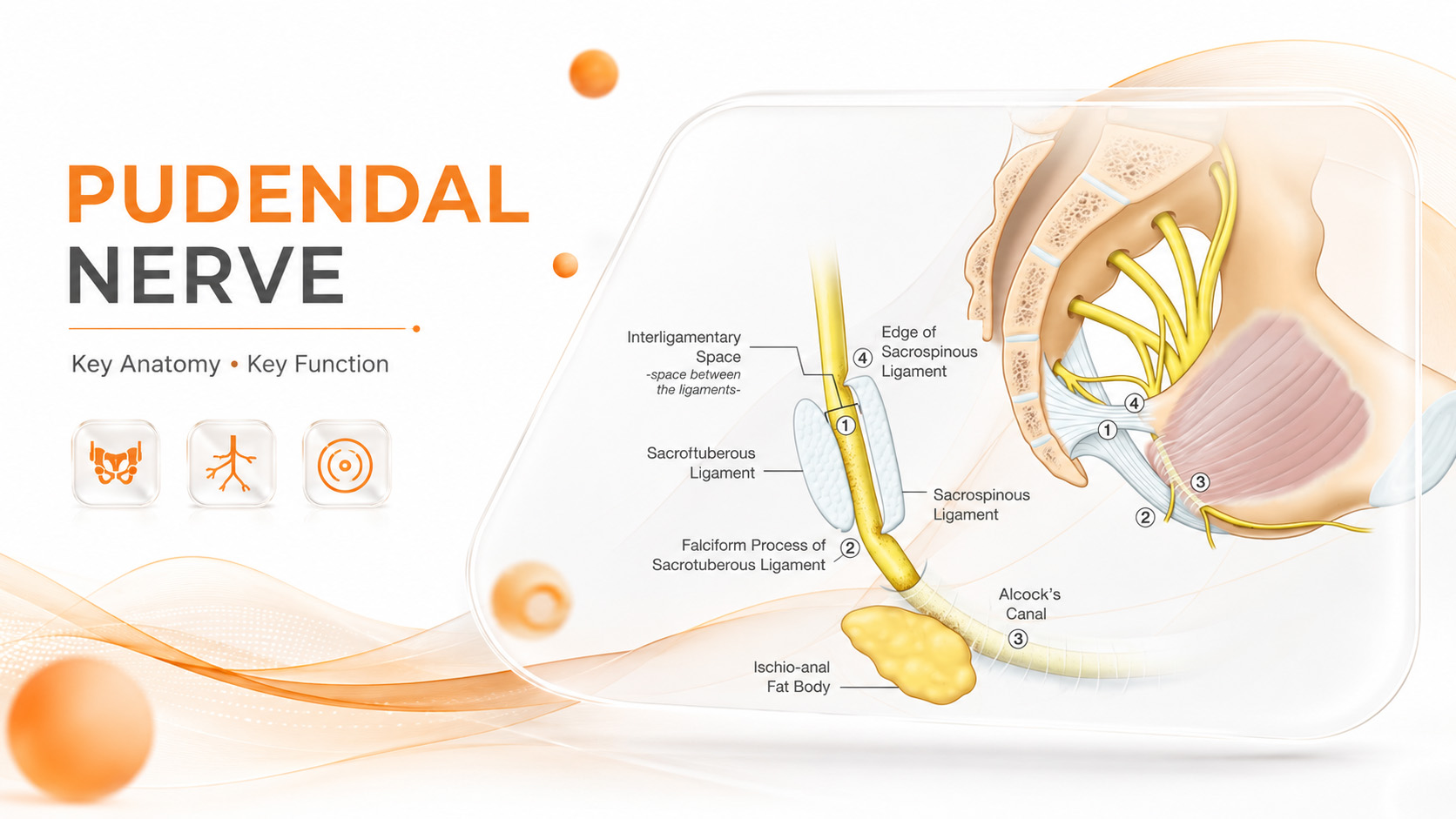
Pudendal Nerve Entrapment
Years of chronic pelvic pain, burning that worsens when sitting, and "treatment-resistant prostatitis / cystitis" often hide an underlying pudendal nerve entrapment. Prof. Dr. Tibet Erdogru is the first surgeon worldwide to describe laparoscopic pudendal nerve decompression.
- World’s first laparoscopic pudendal surgery (2014)
- da Vinci robotic decompression since 2021
- Cases reporting 90% pain reduction

Prof. Dr. Tibet Erdoğru
Quick Application
Leave your details and we will get back to you shortly.